
Meet the team behind your integrative oncology care: Synthesis Clinic at the SIO Europe 2026 Congress
Written by Dr Nina Fuller-Shavel
In May 2026, the integrative oncology community gathered in Rome for the 2nd SIO Europe Congress, held under the theme "From Ancient Wisdom to Modern Integration." Members of the Synthesis Clinic team were there throughout, contributing across the scientific programme and sharing how a coordinated, multidisciplinary team delivers integrative cancer care in practice.

Synthesis Clinic team at the SIO Europe 2026 Congress in Rome
When you are living with a cancer diagnosis, the people around you matter as much as the plan itself. At Synthesis Clinic, integrative oncology is not a single therapy or a single practitioner. It is a coordinated team of doctors, dietetics and nutrition professionals, an integrative clinical pharmacist, nurse prescribers and specialist nurses, physiotherapists and cancer rehabilitation specialists, psychologists, coaches, mind-body therapists, herbalists and acupuncturists, working together to build a shared care plan that dynamically fits your needs, alongside your NHS or private cancer treatment.
This article briefly introduces the Synthesis Clinic multidisciplinary team, explains how the different roles connect, and shares crucial scientific programme contributions from our healthcare professionals presented at SIO Europe 2026 in Rome this May.
What integrative oncology actually means
There is a lot of confusing language in this area, so it is worth being precise. The internationally accepted definition comes from a consensus process led by Professor Claudia Witt and colleagues [1]. They defined integrative oncology as a patient-centred, evidence-informed field of cancer care that utilises mind and body practices, natural products, and/or lifestyle modifications from different traditions alongside conventional cancer treatments. The same consensus paper describes how the field aims to optimise health, quality of life, and clinical outcomes across the cancer care continuum and to empower people to prevent cancer and become active participants before, during, and beyond cancer treatment [1].
Two words in that definition do the heavy lifting: evidence-informed and alongside. Integrative oncology is not an alternative to conventional cancer treatment, and it should never ask a patient to choose between the two. Integrative oncology works with surgery, chemotherapy, radiotherapy, immunotherapy, endocrine therapy and other cancer treatment options, adding support from nutrition, lifestyle medicine, mind-body modalities, carefully selected natural products and complementary therapies where the evidence supports them. This distinction sits at the centre of how Synthesis Clinic works, and it ran through every presentation the team gave in Rome.
Why a team and not a single practitioner?
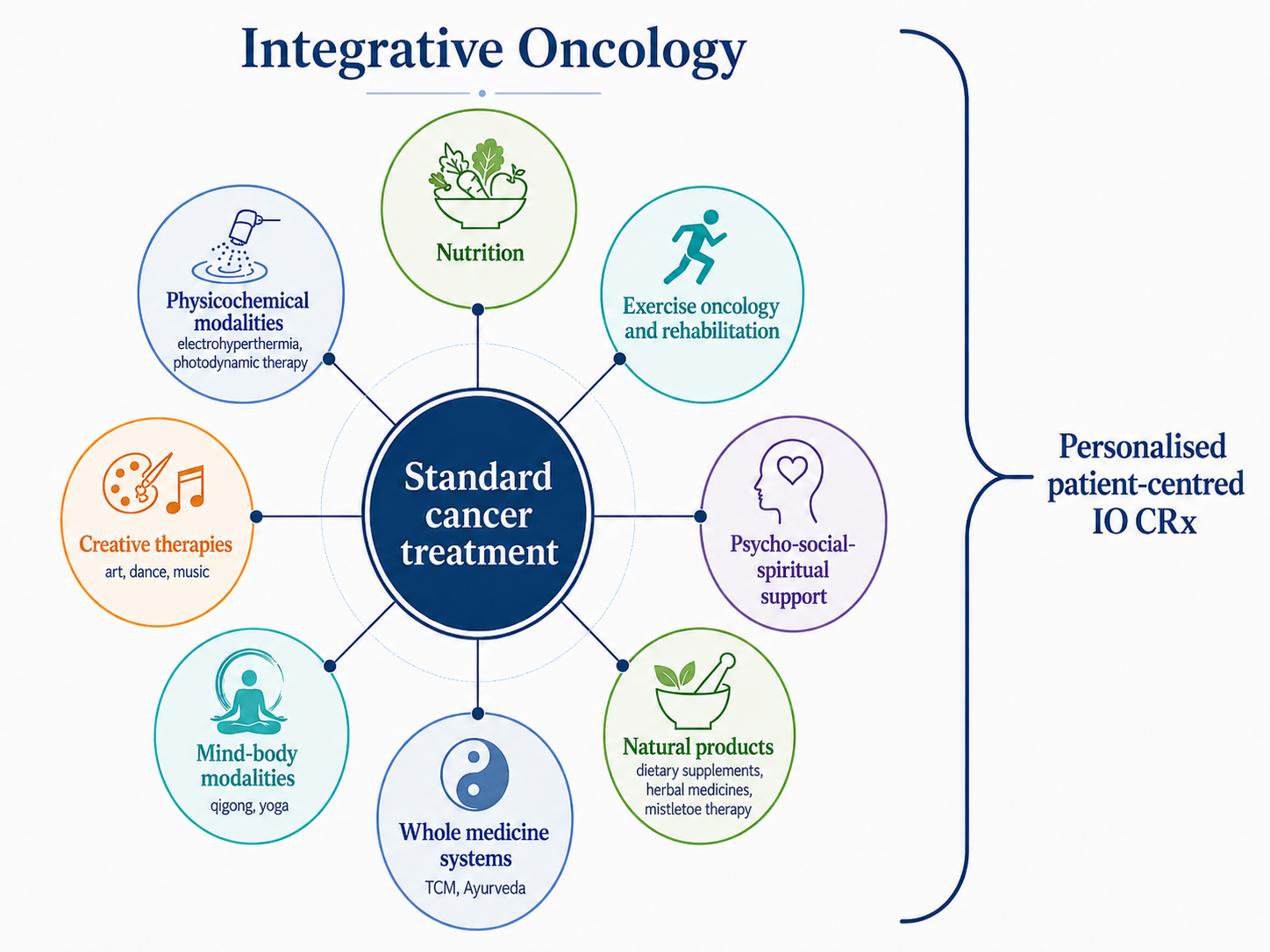
Integrative oncology puts the best of standard of care oncological treatment in the middle and builds around it. By definition integrative is NOT alternative.
Cancer care is rarely about one problem. A person on treatment may be managing fatigue, disrupted sleep, joint pain, low mood, gut symptoms, a long medication list and a great deal of uncertainty, often all at once. No single clinician can address all of that well, even with our Medical Director's many degrees and qualifications. The evidence increasingly shows that combinations of supportive interventions tend to outperform any one intervention used in isolation, a pattern that runs consistently through recent integrative oncology research.
This is why Synthesis Clinic is built as a genuine multidisciplinary team (MDT), a term you may have already encountered in cancer care. Every patient's case submitted to the MDT is reviewed by a physician-led team, with weekly meetings to assess current challenges and progress, including input from our integrated patient-reported outcome measures (PROMs), alongside letters and test results from NHS and private oncology teams. The clinic is CQC-registered, and care is delivered across three specialist service lines (Integrative Cancer Care, Integrative Cancer Pain Care, and Survivorship and Carer Support) that together deliver four MDT meetings a week.
The Synthesis Clinic doctors: medical leadership and whole-person assessment
Dr Nina Fuller-Shavel, Director and Head of Integrative Cancer Care at Synthesis Clinic, presenting at SIO Europe 2026
Integrative oncology at Synthesis is doctor-led. The clinic is directed by Dr Nina Fuller-Shavel, a Cambridge and Oxford-trained physician specialising in precision health and integrative medicine, who also serves as Chair of the Society for Integrative Oncology (SIO) Global Committee and co-authored the international SIO-ASCO guideline on anxiety and depression in adults with cancer [2]. Dr Fuller-Shavel holds degrees in Medicine and Natural Sciences from the University of Cambridge, along with distinctions in an MSc in Precision Cancer Medicine and a PG Diploma in Health Research from the University of Oxford. Alongside her medical training, Dr Nina's qualifications span across nutrition, functional and integrative medicine, herbal medicine, health coaching and yoga, and she integrates this breadth of knowledge seamlessly into both her clinical practice and her teaching and mentoring. Dr Nina Fuller-Shavel is supported by the Synthesis Clinic medical team, including precision health and integrative medicine physicians and consultant specialists across pain medicine and emergency medicine and oncology, including haematological (blood) cancers.
The doctor's role is to hold the whole picture. That means understanding the cancer diagnosis and treatment plan, reviewing symptoms and quality of life, considering lifestyle and precision health information, and building a personalised, written integrative care plan that is then delivered and refined by the wider team. At SIO Europe 2026, Dr Nina Fuller-Shavel served as a Conference Co-President and presented on several areas of this work, including the use of multiomics (specialised multicomponent liquid biopsy analysis) in precision integrative oncology, integrative approaches in breast and ovarian cancer, and integrative oncology as a structured companion to conventional treatment during active therapy, with a specific focus on immunotherapy support.
Integrative cancer pain care: a major focus in Rome
One area stood out in the Synthesis programme at SIO Europe 2026: integrative cancer pain care. Dr Deepak Ravindran, who leads the clinic's Integrative Cancer Pain Care service and is a consultant in pain and musculoskeletal medicine, presented on cancer pain mechanisms and integrative pain care. This is an area where the gap between what patients experience and what conventional care alone tends to offer can be wide, and it deserves explaining properly.
Cancer pain is common and frequently under-treated. Across the cancer population, roughly two in five people live with pain, and the figure is higher in advanced disease and remains substantial among cancer survivors long after treatment ends. Pain also drives a great deal of the wider suffering of cancer, disrupting sleep, mood, energy, and the ability to function and connect with others.
The four kinds of cancer pain
Whole person integrative cancer pain care is the model that targets mixed mechanisms of cancer pain during and after treatment.
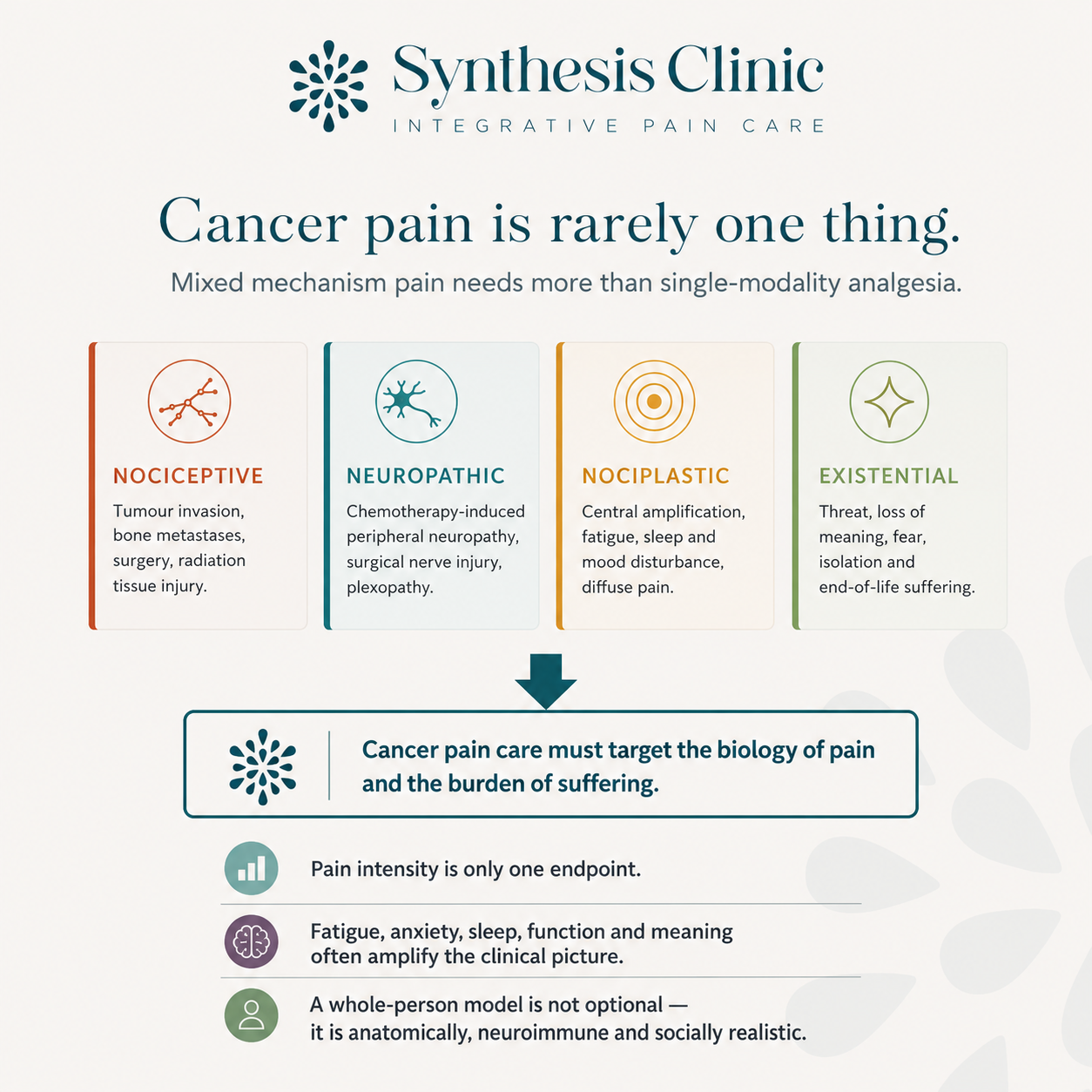
The central message of the Synthesis pain presentation in Rome was simple but important: cancer pain is rarely one thing. It is usually a mixture of different pain types, and that is precisely why a single painkiller, or any single approach, so often falls short. Understanding the mixture is the first step to treating it well.
There are, broadly, four kinds of pain that occur in cancer, and many patients have more than one at the same time. Nociceptive pain comes from direct tissue damage: a tumour pressing on or invading structures, cancer in the bone, or the after-effects of surgery and radiotherapy. Neuropathic pain comes from damage to nerves themselves, such as chemotherapy-induced peripheral neuropathy, nerve injury from surgery, or a tumour affecting a nerve plexus. Nociplastic pain is a newer and less familiar concept: here the nervous system signals become amplified leading to increased sensitivity, a process sometimes called central sensitisation, producing pain that is more diffuse and is closely tied to fatigue, poor sleep and low mood. Studies in breast cancer have found that a substantial proportion of patients have this kind of mixed or centrally amplified pain, and it is frequently missed. Finally, there is what can be called existential pain: the suffering that comes from fear, loss of meaning, isolation and the threat that a cancer diagnosis carries. It is not pain in the tissue sense, but it is very real, it amplifies physical pain, and any honest model of cancer pain has to account for it.
The reason this matters to patients is direct. If pain has four different sources and you only treat one of them, you will only ever get part of the way. Nociceptive pain often responds well to conventional medication and, where appropriate, interventional procedures. But neuropathic, nociplastic and existential pain frequently do not respond fully to medication alone, and that is where a broader, integrative approach earns its place.
How a multidisciplinary team treats pain

Dr Deepak Ravindran, Head of Integrative Cancer Pain Care, at Synthesis Clinic presenting on cancer pain mechanisms in Rome
The integrative model of cancer pain care that Synthesis Clinic presented in Rome treats pain on two fronts at once: the biology of the pain itself, and the burden of suffering that surrounds it. Conventional pain management, including appropriate analgesic medication and, where indicated, interventional procedures such as nerve blocks, remains essential and is never replaced. Around it, the team adds evidence-informed approaches that address the parts of pain that medication alone cannot reach: stress and nervous system regulation, sleep, movement and exercise, nutrition, and mind-body therapies.
The evidence for this broader approach is increasing. The SIO-ASCO clinical practice guideline on integrative medicine for pain management in oncology reviewed a very large body of research and recommends a range of integrative therapies as part of evidence-informed pain care [3]. A 2025 scoping review of integrative cancer pain management screened more than a thousand studies and found that the great majority reported a positive impact on cancer pain, with acupuncture, mindfulness and movement-based therapies among the most promising [4].

Synthesis Clinic offers a consultant-led specialist multidisciplinary care model for cancer-related and treatment-related pain when standard pain management is not enough or is associated with significant side effects.
Some specific signals are worth knowing. Acupuncture has the clearest evidence of the integrative pain therapies: it can reduce pain intensity, may reduce the dose of opioid medication needed, and is recommended for the joint and musculoskeletal pain caused by aromatase inhibitors, a common and quality-of-life-limiting problem for many people on hormone therapy for breast cancer. Mind-body therapies such as mindfulness-based interventions, guided imagery, hypnosis and yoga may work in a different way: rather than switching off pain at its source, they reduce the load the nervous system is carrying, easing the threat, fatigue, poor sleep and anxiety that amplify pain. Massage is recommended in palliative care settings for comfort and quality of life. Carefully chosen supplement approaches may have a role, with proper medical and nutrition oversight, review of supporting evidence and interaction checking.
What makes this work in practice, rather than just in theory, is the team. Treating mixed-mechanism pain well needs a pain physician, but it also needs nurses, physiotherapists, psychologists, and access to acupuncture, mind-body therapies and nutritional input, all coordinated around one plan. That is what an integrative cancer pain service is: not a collection of separate treatments, but a multidisciplinary team treating the whole picture of a person's pain. For many patients, this is the part of integrative oncology that changes daily life the most.
Nutrition and dietetics: food as a core part of the plan

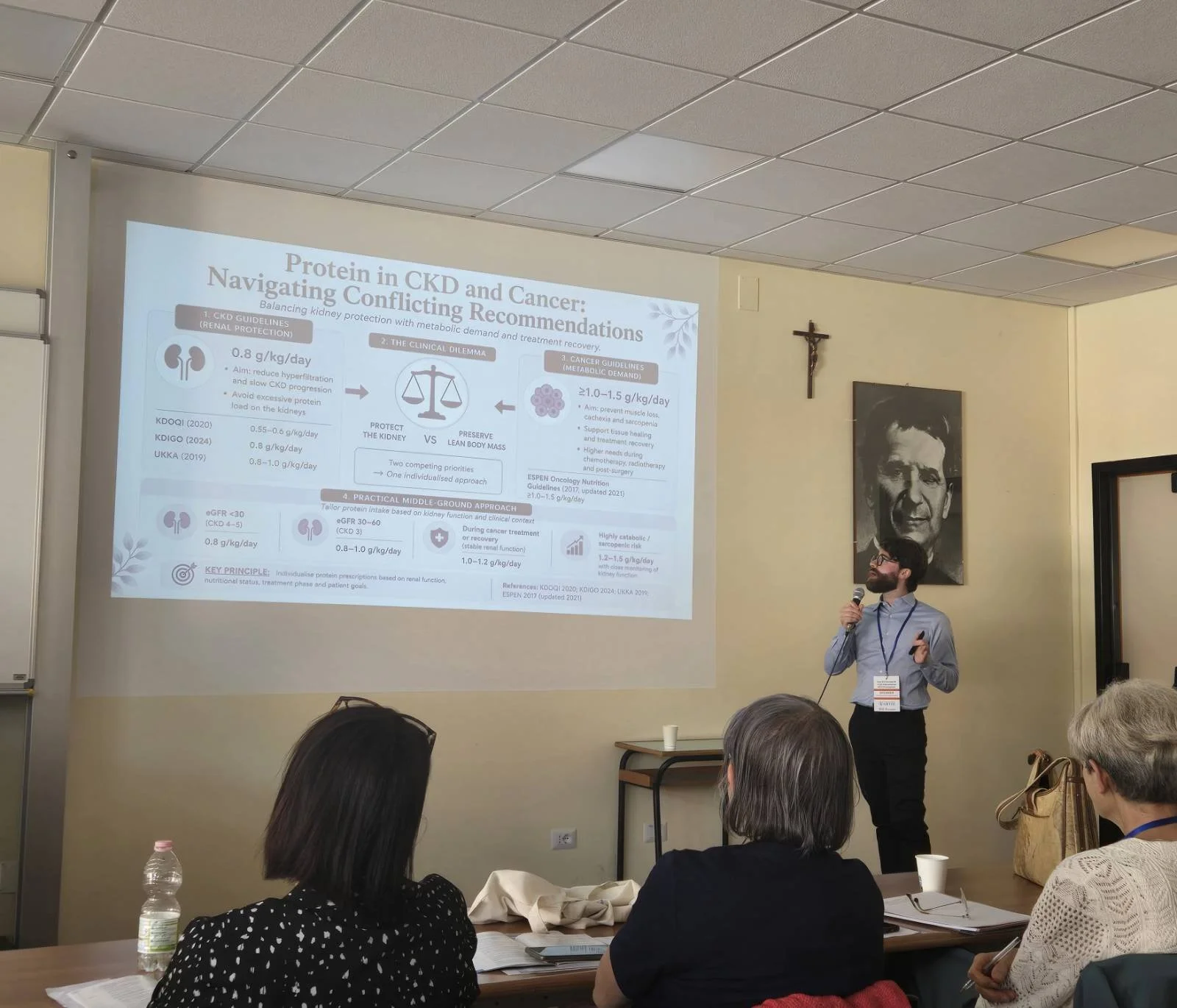
Giuseppe Scapellato - our Renal Dietitian and Cancer Malnutrition Dietitian at Synthesis Clinic
Nutrition is one of the most evidence-rich areas of integrative oncology, and one that patients most often want help with and are confused about. The Synthesis nutrition and dietetics team includes BANT registered nutritional therapy practitioners (RNTPs) and HCPC-registered dietetics input, each able to bring cancer-type-specific and treatment-specific knowledge to a care plan.
A good example of the depth here is Giuseppe Scapellato, a specialist renal dietitian who presented at SIO Europe 2026 on renal protection during and after oncology treatment. Kidney health is an under-discussed part of cancer care, yet for patients on chemotherapy that can be toxic to the kidneys or with pre-existing kidney concerns, it can shape whether treatment continues safely. Having a dietitian with this kind of specialist focus, working inside an oncology MDT, is uncommon in UK practice, but we feel it is a crucial part of wraparound care.
The evidence base supports this attention to nutrition. A 2024 meta-analysis found that pretreatment vitamin D deficiency was associated with around a 50% increase in the odds of a poorer response to neoadjuvant chemotherapy in breast cancer [5]. Vitamin D status has also been linked to chemotherapy-induced nerve symptoms and aromatase inhibitor joint pain, and is crucial in supporting appropriate cancer immunotherapy response [11,12]. None of this means nutrition replaces treatment. It means nutrition is a foundation that, if done well and personalised to you and your therapy plan, properly supports it.
The integrative clinical pharmacist: keeping everything safe
One of the quiet but vital roles in the Synthesis team is that of the integrative clinical pharmacist, Roshni Kothari, who is also the superintendent pharmacist for the new Synthesis Clinic Pharmacy. At SIO Europe 2026 she presented on polypharmacy and medical cannabis in integrative oncology, making a point every patient should hear. In integrative care, the number of things a person is taking, across prescription medicines, including both cancer treatment and supportive care medicines, over-the-counter products, herbal medicines and supplements, can add up quickly, and someone needs to be checking the whole picture for safety and interactions.
This matters because natural does not mean risk-free. Herb-drug interactions are real, and the research presented in Rome highlighted clear examples. Supplemental curcumin, for instance, has shown promising results in some breast cancer studies, yet a randomised pharmacokinetic study found that taking oral curcumin can reduce blood levels of endoxifen, the active form of tamoxifen [6]. While we still do not know how much this impacts the clinical outcome, we would certainly not want to interfere with treatment that may reduce breast cancer recurrence risk without more information. That is exactly the kind of interaction a patient cannot be expected to spot alone, and exactly why integrative pharmacy oversight is built into the Synthesis model rather than left to chance. All our nutrition professionals, herbalists and doctors also conduct careful interaction checks, with Roshni there to support the team. Adding personalised supplements to your regime has to be done both safely and effectively, with scientific evidence, your professional's clinical experience and your unique needs and circumstances in mind.


Nurses and the mobile nursing network: care closer to home
Synthesis Clinic's nursing team, led by Chief of Staff and nurse prescriber, Diogo Madureira, alongside our integrative oncology nurse, Pedro Bessa Pereira, delivers prescribed supportive interventions both at the Reading clinic and, through a mobile nursing network, in patients' own homes across much of England. At SIO Europe 2026, Diogo and Pedro jointly presented on the development of this integrative oncology mobile nursing network.
The reasoning is straightforward. The patients who would benefit most from supportive care are often those for whom travelling to a clinic is hardest, due to fatigue, frailty or distance. A nurse-led, protocol-driven, home-based model, with full medical oversight, helps close that access gap. Every intervention, such as mistletoe therapy, delivered through the network is assessed and prescribed first by a Synthesis Clinic doctor, nurse prescriber or pharmacist prescriber, and reviewed regularly, keeping the same standard of clinical governance wherever care is delivered.
Rehabilitation, mind-body and therapy support
The Synthesis Clinic integrative oncology team also includes physiotherapists, cancer rehabilitation and exercise oncology specialists, clinical psychology and emotional wellbeing coaching, yoga therapy and mindfulness practitioners, medical herbalists and TCM herbalists and acupuncturists. This breadth is deliberate, and it connects directly to the pain work described earlier: many of these practitioners are part of how the clinic addresses the different mechanisms of cancer pain. Recent breast cancer research shows that combined programmes of exercise, nutrition, mind-body practice and selected additional interventions tend to produce the most clinically meaningful improvements, more than any single element on its own.
There is also strong evidence for specific symptom-focused therapies. Fatigue is one of the most common and most limiting problems in cancer, and the SIO-ASCO guideline on the management of cancer-related fatigue recommends approaches including exercise, cognitive behavioural therapy, mindfulness-based programmes and, after treatment, yoga and acupressure and moxibustion [7]. That guidance is borne out by recent trial evidence: a 2026 phase 3 randomised trial published in JAMA Network Open tested app-delivered self-acupressure in ovarian cancer survivors living with fatigue, and found that self-acupressure significantly reduced fatigue compared with usual care, with the improvement sustained months later [8]. For cancer pain specifically, as discussed above, the SIO-ASCO clinical practice guideline reviewed a large body of evidence and recommends interventions such as acupuncture and several mind-body therapies as part of evidence-informed pain management [3].
Personalised microbiome support: an example of the team in action
One area that brings the whole team together is personalised microbiome support, and it was the subject of a Synthesis Clinic abstract selected for the Best of SIO 2026 session in Rome, the congress's showcase of its strongest accepted research. The study was a team contribution, led by Dr Nina Fuller-Shavel as senior author with colleagues including Diogo Madureira and Dr Emma Davies.
The work used advanced stool testing to look at the gut microbiome of patients at different stages of cancer treatment. The science behind this is well established: research published in journals including JAMA and Nature Metabolism has shown that the gut microbiome can influence both how well cancer treatments work and how much toxicity they cause [9,10]. This is an area Synthesis clinicians have written about before. Dr Nina Fuller-shavel has co-authored two peer-reviewed papers on how nutrition and the microbiome can support modern cancer treatment: one with consultant medical oncologist Dr Jonathan Krell on integrative oncology approaches to supporting immune checkpoint inhibitor (immunotherapy) treatment of solid tumours [11], and a 2025 review on nutritional strategies in supporting immunotherapy and other targeted cancer therapies [12].
The Synthesis Clinic audit (currently going through the publication process) found that the microbiome looks measurably different during active treatment compared with survivorship. In a small series of patients with advanced cancer, we observed that personalised, MDT-led interventions, combining dietary changes, specific probiotic strains and other carefully selected support, were associated with meaningful improvements in inflammatory markers, gut microbiome composition and patient-reported symptoms.
It is important to be honest about what this does and does not mean. These were individualised interventions delivered within a physician-led team with full pharmacy oversight, as part of personalised care. The findings come from early, real-world data in a small group of patients, with the full manuscript currently undergoing peer review. The wider field is at a similar stage: the evidence is promising and the direction of travel is clear, but larger studies are still needed. What the work illustrates well is the Synthesis approach in practice: testing where it adds value, interpreting results properly, and translating them into a coordinated plan that several team members deliver together, safely and alongside conventional treatment.
How the team works together
The thread running through all of this, and through everything Synthesis presented in Rome, is coordination. At Synthesis Clinic, a clinic coordinator first encounters any new patient (referred or self-referred) and gets case details, which are then assessed and triaged by the medical team, usually our Medical Director. Where a doctor-led package is commenced, the integrative cancer care physician builds a personalised written care plan, working with other members of the team, such as our nutrition, rehabilitation or emotional wellbeing support professionals. This personalised care plan is discussed at a weekly MDT meeting with physician oversight, screened for drug, herb and supplement interactions by the integrative clinical pharmacist, and then delivered by the relevant team members. Progress is tracked with patient-reported outcome measures and regular review, and the clinic liaises with NHS and private oncology and primary care teams, with the patient's consent, to help coordinate care. If you are not being seen by one of the doctors, your healthcare professional can still always bring your case to the MDT for specific assessment and discussion, so that you can benefit from broader team input.
This is what evidence-informed, patient-centred integrative oncology looks like when it is done properly. Not a collection of separate therapies or 'one-size-fits-all', but one team, one plan, and one shared goal: supporting you as well as possible, alongside the cancer treatment you are already receiving or have undergone.
Learn more about the Synthesis Clinic team
If you would like to understand more about the people who would be involved in your care, you can explore the full team on the Synthesis Clinic website, where each practitioner has their own profile describing their background and special interests, and contact our reception or clinic coordinator team to learn more. You can also read more about the clinic's three services (Integrative Cancer Care, Integrative Cancer Pain Care, and Survivorship and Carer Support) and about how integrative oncology works alongside conventional treatment.
Frequently asked questions
What is integrative oncology?
Integrative oncology is a patient-centred, evidence-informed field of cancer care that combines mind-body practices, natural products and lifestyle approaches with conventional cancer treatment [1]. It is designed to work alongside surgery, chemotherapy, radiotherapy, immunotherapy and endocrine therapy and other cancer treatments, never as a replacement for them.
What is integrative cancer pain care?
Integrative cancer pain care treats cancer pain as the mixed, multi-source problem it usually is. Alongside conventional pain medication and procedures, it adds evidence-informed approaches such as acupuncture, mind-body therapies, movement, sleep support and nutrition, delivered by a multidisciplinary team. The aim is to address both the biology of the pain and the wider suffering around it.
Is integrative oncology the same as alternative medicine?
No. Alternative medicine is used instead of conventional cancer treatment. Integrative oncology is used alongside the best of standard of care and is built with and alongside standard oncology input. Synthesis Clinic only works with patients who are receiving, or planning to receive, appropriate conventional cancer care where this is offered to them. We also help patients access second opinions and clinical trials where needed to ensure that the standard oncological care they receive is the best fit for their circumstances.
Who is in the integrative oncology team at Synthesis Clinic?
The team includes integrative medicine doctors and consultant specialists, a consultant-led integrative cancer pain service, registered dietitians and nutritional therapy practitioners, an integrative clinical pharmacist, nurse prescribers and specialist nurses, physiotherapists and exercise oncology specialists with scar therapy and lymphoedema support training, psychologists and health and emotional wellbeing coaches, medical herbalists and TCM herbalists and acupuncturists, all working together to deliver shared care plans and packages.
Can I receive integrative oncology care at home?
You can do most (if not all) of your consultations online via telehealth if you wish, unless you need to come in for acupuncture or other hands on treatment. If you need specific integrative oncology interventions, such as mistletoe therapy or IV vitamin C, we also have this available at home across most of England. Synthesis Clinic runs a mobile nursing network that delivers prescribed supportive interventions in patients' homes, with full prescriber oversight. The clinic coordinator team can confirm whether the network currently covers your area and let you know how we monitor you during supportive integrative care, such as through regular blood tests and nursing support.
Does integrative oncology have scientific evidence behind it?
Yes. There is a growing evidence base, including randomised controlled trials and society guidelines such as the SIO-ASCO guidelines on pain, anxiety and depression, and fatigue [2,3,7]. The strength of evidence varies by intervention, and a core principle of the Synthesis approach is being honest about what the evidence does and does not yet show and tailor the approach to you.
How do I find out if Synthesis Clinic is right for me?
The best first step is to learn more about the team and services is here on the Synthesis Clinic website. From there you can see how the multidisciplinary model works and decide whether it fits what you are looking for, and contact our reception or clinic coordinators to discuss further.
This article is for general information and patient education. It is not medical advice and does not replace consultation with your own medical team. Always discuss any changes to your care, including supplements, herbal medicines or lifestyle changes, with your oncology team or a qualified and registered clinician.
References cited in this article are drawn from peer-reviewed literature. The Synthesis Clinic microbiome study referred to was presented at the 2nd SIO Europe Congress (Rome, May 2026), and the full manuscript is currently undergoing peer review. It is therefore not cited here and should not be reproduced without the authors' permission until it is available in the public domain.
About the author
Dr Nina Fuller-Shavel is the founder and Director of Synthesis Clinic, an award-winning multidisciplinary integrative oncology practice in the UK. She is an Oxbridge-trained integrative medicine doctor, scientist and educator with over a decade and a half of experience in integrative healthcare, and a Fellow of the College of Medicine, the British Association for Nutrition and Lifestyle Medicine (BANT) and the Royal Society of Arts (RSA). Alongside her degrees in Medicine and Natural Sciences from the University of Cambridge and and MSc in Precision Cancer Medicine and PG Dip in Health Research from the University of Oxford, Dr Fuller-Shavel holds multiple qualifications across nutrition, integrative and functional medicine, health coaching, herbal medicine, Traditional Chinese Medicine, yoga and mindfulness. She is co-author of Integrative Oncology in Breast Cancer Care (Springer, 2024) and actively contributes to integrative oncology research, scientific journal editorial boards and international guideline development. Dr Fuller-Shavel’s research and clinical practice centre on integrative approaches to immunotherapy across multiple cancer types, specialist support for breast and gynaecological cancer, and the role of the gut microbiome in cancer care, with a focus on improving treatment outcomes, easing side effects and supporting quality of life, working alongside conventional oncology care.
References
1. Witt CM, Balneaves LG, Cardoso MJ, Cohen L, Greenlee H, Johnstone P, et al. A comprehensive definition for integrative oncology. J Natl Cancer Inst Monogr. 2017;2017(52):lgx012.
2. Carlson LE, Ismaila N, Addington EL, Asher GN, Atreya C, Balneaves LG, et al. Integrative oncology care of symptoms of anxiety and depression in adults with cancer: Society for Integrative Oncology-ASCO guideline. J Clin Oncol. 2023;41(28):4562-4591.
3. Mao JJ, Ismaila N, Bao T, Barton D, Ben-Arye E, Garland EL, et al. Integrative medicine for pain management in oncology: Society for Integrative Oncology-ASCO guideline. J Clin Oncol. 2022;40(34):3998-4024.
4. Bell BK, Cha J, Cavanaugh KA, et al. Integrative management of cancer pain: a scoping review of the literature. Cancer Med. 2025;14(9):e70833.
5. Shu C, Yang Q, Huang J, Xie X, Li H, Wu H, et al. Pretreatment plasma vitamin D and response to neoadjuvant chemotherapy in breast cancer: evidence from pooled analysis of cohort studies. Int J Surg. 2024;110(12):8126-8135.
6. Hussaarts KGAM, Hurkmans DP, Oomen-de Hoop E, et al. Impact of curcumin (with or without piperine) on the pharmacokinetics of tamoxifen. Cancers (Basel). 2019;11(3):403.
7. Bower JE, Lacchetti C, Alici Y, Barton DL, Bruner D, Canin BE, et al. Management of fatigue in adult survivors of cancer: ASCO-Society for Integrative Oncology guideline update. J Clin Oncol. 2024;42(20):2456-2487.
8. Zick SM, Chen D, Harris RE, Kruger G, Runyon A, Sen A, et al. Self-acupressure for fatigue in patients surviving ovarian cancer: a randomized clinical trial. JAMA Netw Open. 2026;9(2):e2556357.
9. Fernandez E, Wargo JA, Helmink BA. The microbiome and cancer: a translational science review. JAMA. 2025;333(24):2188-2196.
10. Nobels A, van Marcke C, Jordan BF, Van Hul M, Cani PD. The gut microbiome and cancer: from tumorigenesis to therapy. Nat Metab. 2025;7(5):895-917.
11. Fuller-Shavel N, Krell J. Integrative oncology approaches to supporting immune checkpoint inhibitor treatment of solid tumours. Curr Oncol Rep. 2024;26(2):164-174.
12. Fuller-Shavel N, Davies EJ, Peleg Hasson S. Nutritional strategies in supporting immune checkpoint inhibitor, PI3K inhibitor, and tyrosine kinase inhibitor cancer therapies. Front Nutr. 2025;12:1670598.